Dentistry is faced with a number of market and professional challenges that are leading to a “perfect storm” of circumstances impacting complete denture fabrication. The complete denture clinical protocol has changed little over the past 50 years. The traditional five-appointment denture protocol is still being taught by a majority of dental schools. However, less curriculum emphasis is being placed on denture fabrication techniques and there are fewer complete denture cases completed during typical dental education.1
Similarly, little has changed in the basic procedures used by dental laboratories to fabricate dentures. Although denture teeth and precision processing techniques have been improved, the techniques that have been in practice for decades remain largely the same. Polymerization shrinkage continues to be an ongoing and confounding problem affecting both fit and occlusion.2,3
Many dentists choose not to treat fully edentulous patients out of a lack of confidence in their clinical technique and concern over achieving a predictable outcome for their patients (David A. Avery, CDT, personal communication, January 2014). Denture patients can be difficult to please and often have unreasonable expectations.4,5 Accurate and thorough impressions seem somewhat arbitrary and require a skilled clinician to achieve.6 Bite registration, too, can be a vexing challenge.
Further adding to the problems associated with providing dentures to patients who need them, there is a shortage of qualified, experienced denture laboratory technicians.7 Several laboratory technology programs have closed across the United States, and among those technicians best qualified to produce dentures, the average age is over 50.8
In less than a decade, CAD/CAM technology has become a dominant factor in the day-to-day dental laboratory workflow, primarily related to crown and bridge and implant-related prostheses.9 Recently, there has been development of viable digital denture fabrication processes, one of which is featured in this case report. Heraeus Kulzer (heraeus-kulzer-us.com) has developed a new clinical and laboratory workflow called the Pala Digital Denture. This system is a combination of new laboratory CAD/CAM technology and a recently introduced clinical workflow for use with edentulous patients. Heraeus utilizes a combination of clinical data and a carefully documented computer algorithm based on anthropometric averages to produce a complete denture prosthesis.10
Rather than scheduling separate appointments for impressions and jaw relation, the clinician can accomplish both in a single appointment. This is aided by a unique impression tray system and the use of a central bearing device, which is a well-proven method for obtaining centric relation bite records.11,12 The clinical documentation is then sent to the local laboratory for scanning and processing. Next, the Heraeus Pala center receives the scan files, along with photographs and a complete checklist of clinical documentation. The processing center then manipulates the data within its system and develops a proposal for the intended prosthesis using 3D printing technology to develop a digitally manufactured denture try-in. This try-in is returned to the dentist for a traditional denture try-in appointment.
After the try-in is clinically accomplished, significant findings are recorded, as is photography if necessary. An extensive, detailed checklist of modifications facilitates communication with the Pala manufacturing facility, and offers ample opportunity for constructive feedback for the final restoration. It is not necessary to return the printed try-in unless a new bite registration is required. However, it is important to be aware that the printed try-in requires some getting used to. It is a monochromatic, very white duplicate of the intended denture (Figure 1). The very nature of the color makes it a bit challenging to evaluate for both patient and doctor.
Patient Case
A 55-year-old female presented with an extensive history of health issues, including cancer treatment 10 years earlier; however, based on consultation with the patient’s physicians, there were no contraindications for dental treatment. The clinical examination revealed an ill-fitting, highly unesthetic upper denture and a few remaining unrestorable mandibular teeth and root tips (Figure 2). It was observed that the patient had highly mobile perioral musculature. In addition, she provided 30-year-old photographs (Figure 3) that showed maxillary excess leading to a very “gummy” smile. The patient had reasonable treatment expectations.
Treatment Plan
The treatment plan entailed extracting the patient’s remaining mandibular teeth and allowing an 8-week healing period, after which surgical treatment results could be re-evaluated before proceeding with full dentures using the Heraeus Kulzer Pala digital denture protocol.
Clinical Technique
The Pala denture kit comes complete with segmented impression trays that have a slot assembly uniquely designed to support a central bearing device (included). In addition, the kit provides scannable PVS impression materials, bite registration materials, and a complete array of clinical support documentation.13
The clinical protocol consists of fitting the impression trays based on the basic size of the patient’s edentulous arches. Once selected, the trays can be modified both with heat and by removal of any excess tray material with a lab bur. An initial impression is taken with the material to develop border moulding and establish stable stops for the final wash impression. The first impression is evaluated for any over-extensions and/or impingements on the intaglio surfaces. These issues are managed prior to a final thin wash of scannable PVS impression material. There are extensive instructions on how to develop these impressions in the clinical reference guide.
Once impressions are accomplished, there is a cut line built into the trays. The mandibular retromolar pads and the maxillary hamular notch area are sectioned away from the impression trays. This is done to ensure that bite registration procedures can be accomplished without any posterior interferences. A central bearing device is fit into the tray slots engineered to support both the guide and the table used for defining centric relation. The truncated trays with their respective central bearing device components are inserted in the mouth. The central bearing device has an adjustable screw that defines the vertical dimension at which the case will be fabricated. Vertical is determined using pretreatment measurements, facial profile, and general facial indications.
The patient is instructed to go through protrusive and lateral excursions. The self-adhesive inked sheet provided leaves the distinctive “crow’s foot” range of mandibular motion. The point of the foot marking is defined as centric relation. A small dimple is cut at the point to stabilize jaw position by holding the guide pin in a repeatable reference position. Bite registration material is injected to record the inter-jaw relationship with sufficient material to stabilize the trays (Figure 4). All clinical information checklists are completed and sent along with patient photography to the Pala Denture Processing Center.
The printed digital try-in was returned for clinical evaluation and patient approval (Figure 1). Its basal seat and occlusion were excellent. Minor changes were requested via photography and the checklist for feedback.
Treatment Outcome
Denture delivery was efficient and consisted of evaluating the basal seat, occlusal relationship, and esthetics. The dentures inserted with a satisfying sound of suction being developed, on both arches. Both dentures were very stable. Pressure-indicating paste revealed no pressure spots. Occlusion was evaluated both visually and with articulating paper. Contacts were equal and well distributed. When phonetics were evaluated, some slight lisping was evident, but it was not considered excessive, and proved to be nearly nonexistent at the 3-day recall. (It should be noted that the patient had never worn a lower denture.)
Although the patient’s mobile musculature and maxillary excess did result in a somewhat “gummy” smile, she was extremely positive about the esthetic result, and further reported total comfort and satisfaction on the day of delivery.14 The 3-day re-care appointment was uneventful. One small sore spot was adjusted. The patient was enthusiastic about the experience. The basal seat of the dentures was considered exceptional, occlusion was stable, and the esthetics were deemed more than satisfactory (Figure 5).
Summary
This case study represents what may prove to be the future of complete denture prosthetics. The simplified, yet accurate, clinical technique is easily learned and implemented. It eliminates at least two of the traditional appointment steps in clinical denture fabrication. There is ample opportunity to evaluate the case with the printed digital try-in. This try-in can be modified by taking new bite registrations or even retaking one or both impressions if needed prior to development of the final appliances. The laboratory workflow is driven by CAD/CAM and eliminates many of the techniques that traditional denture fabrication requires, along with the emphasis on seasoned technicians.
Conclusion
In closing, the Pala Digital Denture provides solutions to many contemporary challenges encountered with traditional denture fabrication protocol. A simplified clinical technique that is easy to learn and understand along with a predictable delivery will appeal to many dentists. The accuracy of CAD/CAM dentures eliminates polymerization shrinkage and subsequent issues with the occlusion and fit of appliances. This workflow may well prove to be an answer to the aforementioned “perfect storm” of circumstances. Technology can reduce the need for skilled technicians, provide confidence for clinicians, and generally streamline the entire denture fabrication process.
A Helping Hand: Pala Digital Dentures
Your hands help restore patients to good health. See the videos below to understand how Heraeus Kulzer can help you do just that.
Pala Digital Dentures - Benefits
Better fit, faster production, higher profitability—watch how Pala Digital Dentures is the perfect way to expand your bottom line and services.
insidedentaltech.com/go/idt792
Pala Digital Dentures - 3D Scanning
Pala Digital Dentures utilizes cutting-edge 3D software to provide increased accuracy and more comfortable dentures, and allows a case to be completed twice as fast.
insidedentaltech.com/go/idt793
Pala Digital Dentures Solutions
See the blueprints for successful patient outcomes and then build a bigger profit margin.
insidedentaltech.com/go/idt794
A video from the author
Larry R. Holt, DDS, interviews his patient about how Pala Digital Dentures exceeded her expectations.
insidedentaltech.com/go/idt795
Acknowledgment
The author would like to thank the team at Heraeus Kulzer and Drake Precision Dental Laboratory in Charlotte, NC, where work was mediated. Without their help, this exemplary case could not have been accomplished.
Disclosure
Larry R. Holt, DDS, received material support and an honorarium from Heraeus Kulzer.
About the author
Larry R. Holt, DDS
Director of Clinical Education and Research
Drake Precision Dental Laboratory
Adjunct Faculty
UNC School of Dentistry
Chapel Hill, North Carolina
References
1. Petropoulos VC, Rashedi B. Complete Denture Education in U.S. Dental Schools. J Prosthodont. 2005;14(3):191-197.
2. Wong DM, Cheng LY, Chow TW, Clark RK. Effect of processing method on the dimensional accuracy and water sorption of acrylic resin dentures. J Prosthet Dent. 1999;81(3):300-304.
3. Kawara M, Komiyama O, Kimoto S, Kobayashi K. Distortion behavior of heat-activated acrylic denture-base resin in conventional and long, low-temperature processing methods. J Dent Res. 1998;77(6):1446-1453.
4. Beck CB, Bates JF, Basker RM, Gutteridge DL, Harrison A. A survey of the dissatisfied denture patient. Eur J Prosthodont Restor Dent. 1993;2(2):73-78.
5. Yoshizumi D. An evaluation of the factors pertinent to the success of a complete denture service. J Prosthet Dent. 1964;14(5):866-878.
6. Duncan JPEG, Taylor TD. Teaching an abbreviated impression technique for complete dentures in an undergraduate dental curriculum. J Prosthet Dent. 2001;85(2):121-125.
7. Christensen G, Yancey WR, Schoenbaum TR. The mounting challenges facing the lab industry and the effects on clinical practice. Dental Economics. 2013;103.1
8. Zamanian K, Wong J. New technologies guide paradigm shifts in dental prosthetics industry. Business USA. Jan. 30, 2012. Dental Tribune Website. https://www.dental-tribune.com/articles/business/usa/7335_new_technologies_guide_paradigm_shifts_in_dental_prosthetics_industry.html. Accessed February 2, 2015.
9. Cohen A. Digital Technology and the Future of Dentistry Using cutting edge production methods to create industry leading restorations. Inside Dental Technology. 2013;4(10):72-73.
10. Sawiris MM. The role of anthropometric measurements in the design of complete dentures. J Dent. 1977;5(2):141-148.
11. el-Gheriani AS, Winstanley RB. The value of the Gothic arch tracing in the positioning of denture teeth. J Oral Rehabil. 1988;15(4):367-371.
12. Massad JJ, Connelly ME, Rudd KD, Cagna DR. Occlusal device for diagnostic evaluation of maxillomandibular relationships in edentulous patients: a clinical technique. J Prosthet Dent. 2004;91(6):586-590.
13. Drago CJ. A retrospective comparison of two definitive impression techniques and their associated postinsertion adjustments in complete denture prosthodontics. J Prosthodont. 2003;12(3):192-197.
14. Alfadda SA. The relationship between various parameters of complete denture quality and patients’ satisfaction. J Am Dent Assoc. 2014;145(9):941-948.
Figures and Images

Figure 1

Figure 2

Figure 3
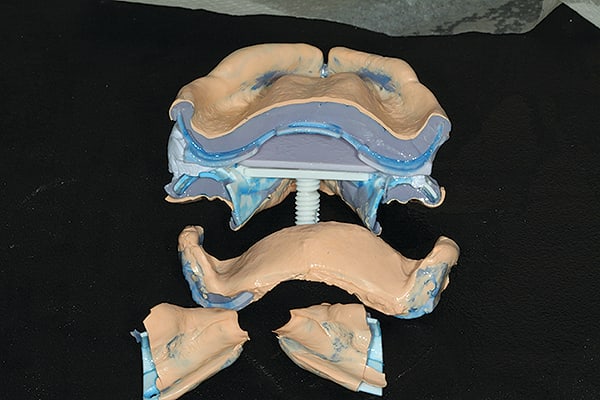
Figure 4

Figure 5
